

Disrupting Big Pharma
“Pfizer Expects $33.5 Billion In Vaccine Revenue In 2021”
“AstraZeneca sales of Covid vaccine triple to $1.2bn in first half of 2021”
These randomly collected headlines give an indication of how much profit will be earned this year by Big Pharma companies in response to COVID, and it seems set to continue ad infinitum. This will place a level of burden on global healthcare systems never before imagined, or budgeted for, by any Government.
Even before this, the Tuft’s University estimate for the cost to develop a new drug was $2.6 billion. This has been used, in part, to justify the price of new drugs coming to market, for conditions such as blood cancers, at nearly $300,000 per treatment.
It is vital, therefore, that we look behind the veil of secrecy that prevents the ordinary person understanding what merits such stupendous rewards, when no other industry even comes close.
By the end of this article, you will have all the facts and evidence you need to be able to judge the fairness, or otherwise, of this. Then you can ask yourself “Do politicians need to step in?”
It wasn’t always like this
Many will not be aware that the industry was not always structured the way it is now. Prior to the early 1980s, large pharmaceutical companies were the alpha male of the industry. They owned nearly every asset and skillset required to discover, develop, manufacture, and distribute drugs into healthcare systems.
I first joined the industry in 1980 working in manufacturing and supply for a Bayer AG site in Wales. The sourcing, manufacturing and supply process was fully integrated, from the point where raw materials arrived at the back door and the finished product was made and sent directly to customers—hospitals, pharmacies and sometimes patients at home.
Links with customers were therefore direct, and our staff would handle customer complaints. The folk making Alka Seltzer for Europe had a standing joke. A polystyrene packing piece was at the top of each glass bottle as a cushion to prevent the tablets from moving and breaking. It was not unusual for customers to send the piece back to the plant with a complaint that it wouldn’t dissolve. The reply was always polite and understanding, but it was hard to resist a wry smile.

Suddenly, it all changed
In November 1976, Smith Kline & French (SK&F – now GSK) had launched Tagamet, a prescription-only drug (drug or drugs from here on) to combat stomach ulcers. It quickly took off and was dubbed the world’s first ‘blockbuster’ drug (≥ $1 billion annual sales).
Glaxo (now GSK) launched a competitor product, Zantac, in 1981 and immediately targeted reportedly minor side-effects of Tagamet to pitch their case to doctors. By 1987, Zantac had become the world’s biggest-selling prescription drug, outselling Tagamet 3:1 at one point.
This was the first example of clever targeting capturing competitor markets, and it stimulated phenomenal growth in the therapeutic area; the profits were immense for both companies, on sales of tens of billions of dollars. The beginning of a perceived lucrative strategy for the industry was cast.
Outsourcing non-core assets and activities begins
About the same time, other sectors were outsourcing ‘non-core activities’, in a move to transfer risk of failure into the supply-base and reduce the fixed costs tied up in employing people and owning facilities. In the light of Glaxo’s marketing success, the new strategy was to focus on discovery research and sales & marketing, categorising them as core activities. The following were classified as non-core activities:
Pre-clinical development (eg safety testing)
Running and administering clinical trials
Manufacturing materials for clinical trials and commercial supplies
Servicing pharmacies and clinics with finished products.
A cull then took place, with masses of workers shown the door and thousands of facilities sold off. Some of the redundant executives set up their own small companies to develop drugs. Other exiting executives bought up facilities to provide these small drug developers with the services above, in exchange for a fee.
These became known as contract development and manufacturing organisations (CDMOs) and contract research organisations (CROs).
Warehousing and distribution assets supplying hospitals and pharmacies were sold off to wholesalers who are now the patients’ link with their medicines and healthcare products. There is very little, if any, conversation between Big Pharma and wholesalers.
Finally, perfectly viable products were dropped because they did not meet the sumptuous return on investment targets. They were picked up by what is now the generics industry. Today, the vast majority of drugs are supplied by the generics companies working to tight margins.
In summary, not to put too fine a point on it, Big Pharma is a dried-up prune compared to the fulsome plum it used to be. It has retrenched into opposite ends of the prescription drug lifecycle, leaving most of the physical work to third party contractors.
The complexity of this structure cannot be overstated. The number of actors involved in the supply chain is immense, making it very difficult to know who is doing what.
What has resulted from this excursion into outsourcing?
The words of Professor Andrew Cox, a world leading authority on procurement and outsourcing best practice, describe the impact of the change:
“Unfortunately for the major pharmaceutical companies that used to be the “channel captains” who controlled the industry and all its major supply chains through a judicious control internally of critical assets, there has been considerable evidence of very poor practice in outsourcing in recent years. This has led to the loss of critical assets, post-contractual moral hazard and poor post-contractual management of suppliers.”
Those are sobering words from Professor Cox. In simple terms, he is saying that Big Pharma companies have little direct involvement in the supply chains they hold responsibility for. Given that the end-to-end supply chain produces and delivers the drugs that are administered to patients, alarm bells should be sounding right now.
What went wrong?
In Figure 3 we see there are three key milestone dates in the life of a drug—patent award, regulatory approval, and expiration of the patent (20 years from award): and two broad phases—product development and market exploitation.
Figure 3 Key milestones in the life of a patented drug
Big Pharma companies focussed on patenting molecules (compounds) and exploiting the market post-approval. As we heard above, developing products was handed over to third party contractors with no skin in the game, other than meeting the terms of their contracts—that’s business of course.
Readers may ponder on the implications of this before we move the analysis forward.
Did Big Pharma take the wrong fork in the road?
Yes, rather than focus on patents and sales & marketing, it should have taken a leaf out of the SK&F book, the background to which you are about to hear.
In 1964, SK&F set up an acid secretion programme in its UK arm, with a vastly experienced team from across the drug development disciplines. They were pioneers of rational drug design, whereby a drug was designed based on knowledge of a biological target known as a receptor. This was in contrast to the industry tradition of trial-and-error testing according to the serendipity principle.
Over the pond at SK&F was another set of individuals developing the PROCESS to make the drug as a commercial proposition. This in-company collaboration was reported to have worked incredibly well.
One account, by the American Chemistry Society (ACS) commented on the development effort “[this] is a story of single-minded commitment by a group of creative scientists working in close collaboration in the United Kingdom. The process of research and development for economical production of the resulting drug, cimetidine [Tagamet], was the work of equally creative scientists working in the United States.”
The head of the cimetidine programme, Sir James Black, later received the Nobel Prize for his drug research.
Sir David Jack, who was responsible for Glaxo’s development effort in bringing Zantac to market in only 5 years, was quoted as saying:
“The development of Zantac had not been in the same order of inspired breakthrough as the research which produced Tagamet… It’s not necessary to shake the earth on its axis to make money in this industry. We simply improved on James Black’s product by choosing a substance with a cleaner reaction.
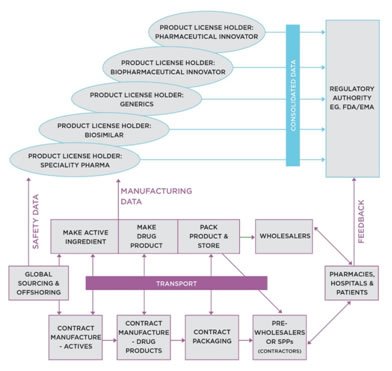
So, if Big Pharma eyes had instead landed on SK&F’s integrated approach to product development, rather the profit potential of the patent, it could all have been so very different. Sadly, that was not the case, and we are living with the picture we see in Figure 2 above.
Is it too late to turn this around?
No, it certainly is not, although there is at least a generation of change required, as the broken system responds to well thought out Government policy, based on a sound understanding of Systems Thinking.
Russell Ackoff, world famous Systems Thinker, had wise words for Politicians to draw on if they wish to make a difference in the world of medicines:
“Don’t fight the system, change the rules and the system will change itself”
The first step in rules change should be to consult on, review and reform the rules on patent law applicable to medicines. Today, a patent is awarded on the back of a biological theory (mode of action), a chicken wire diagram of a molecule, and testing of a few grams of compound made in a laboratory. That then allows a company to ‘claim’ a molecular compound as their own, even though they have no clue if it will ever get to market.
In fact, only one in 10,000 patented molecular compounds get to market. This means of the $2.6 billion claimed to develop a drug, at least $2.0 billion is the cost of failed pre-clinical and clinical studies that did not fulfil the initial potential.
Could Politicians change this?
Indeed, they could, by campaigning for changes to patent law that require more evidence of safety, efficiency and manufacturability before a patent is awarded. The predictive technologies exist, but there is little appetite to use them, preferring the old tried and tested 50-year-old methods.
To make this work, Regulatory Authorities, for example FDA (US)/EMA (EU)/ PMDA (Japan), must become an essential part of the process that considers patent applications, as only they have the necessary skills and experience to judge the evidence provided.
There is already a political move to address high drug prices due to patents in the US, where a letter penned by senior US Senators and Congress Members has been sent to the U.S. Patent and Trademark Office
It is vitally important that Politicians globally get behind this initiative, as current patent law has driven Big Pharma and the industry to where things are today, as described above.
Time for Politicians to step in!